Medical Coatings: Biocompatible Applications of Ti, Ta & Oxide Targets
The human body is the most corrosive environment in engineering.
Salt. Heat. Constant motion. Aggressive proteins. And zero tolerance for failure.
A hip replacement that fails after five years, not twenty, is rarely due to the bulk material.
It is almost always a surface problem. For medical implants and precision surgical tools, the coating is not a finish. It is the interface between device and patient, and everything else depends on it.
This article examines how coating selection — with titanium, tantalum, their oxides, and diamond-like carbon — determines clinical outcomes in orthopedics, cardiology, and surgical instrumentation.
1. The Clinical Landscape: Where Coatings Matter
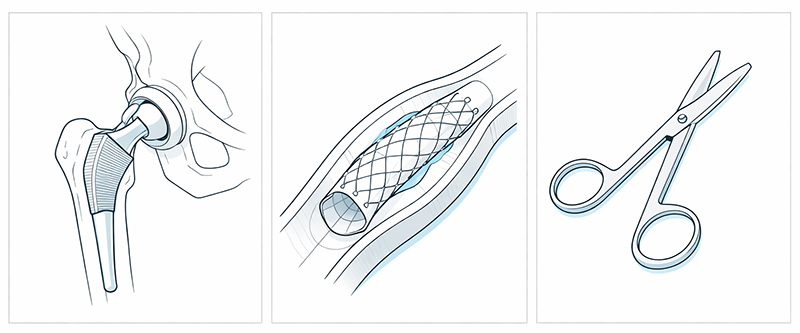
In orthopedic reconstruction, a hip or knee replacement must withstand three to five times body weight. It must endure millions of cycles each year. The failure mode most surgeons fear is wear debris: particles generated at the bearing surface that trigger an inflammatory cascade, leading to osteolysis and eventual loosening of an otherwise well-fixed implant. The coating on the bearing surface is the first line of defense against this process.
In cardiovascular applications, the environment is no less demanding. A coronary stent contacts blood at 70 to 80 beats per minute, day and night, for the life of the patient. Restenosis, thrombosis, and corrosion fatigue are the enemies, and the coating — whether passive oxide or drug-eluting polymer — must remain intact and hemocompatible through millions of deformation cycles.
For surgical instruments, the challenge is repeated sterilization. Autoclave, plasma, and chemical sterilizers attack surfaces aggressively. Corrosion pitting, edge dulling, and tissue adhesion are daily frustrations in the OR. The right coating preserves cutting geometry, resists corrosion, and releases tissue cleanly — case after case, cycle after cycle.
2. What the Body Demands
Biocompatibility is the threshold requirement, and it is non-negotiable. The ISO 10993 series governs biological evaluation, covering cytotoxicity, sensitization, irritation, and systemic toxicity. ASTM F86 defines how surfaces must be prepared and cleaned before coating. No amount of mechanical performance justifies a material that the body rejects.
Wear resistance comes next. For hip bearings, ISO 14242 requires simulator testing to five million cycles minimum, with wear rates below one cubic millimeter per million cycles as a typical target. The coating must survive without delamination, without generating third-body wear particles, and without degrading over time.
Corrosion resistance is equally critical. Physiological saline at 37 degrees Celsius and pH 7.4 is aggressively corrosive, and proteins only complicate the electrochemistry. Pitting potential must exceed anything the body can deliver, and oxide stability determines whether metal ions release into surrounding tissue.
Adhesion to the substrate ties everything together. A coating with perfect biocompatibility and wear resistance is useless if it spalls off at the first load. Scratch testing per ASTM C1624 typically requires critical loads above 30 newtons for medical coatings, and achieving that demands scrupulous attention to substrate preparation — surface energy, cleanliness, and activation all play their part.
| Requirement | Typical Target | Test Method |
|---|---|---|
| Biocompatibility | ISO 10993 pass | Cytotoxicity, sensitization, irritation |
| Wear rate | < 1 mm³/million cycles | ISO 14242 (hip simulator) |
| Adhesion critical load | > 30 N | ASTM C1624 (scratch test) |
| Surface roughness (blood contact) | < 10 nm Ra | AFM, profilometry |
| Corrosion resistance | No pitting in saline | Potentiodynamic polarization |
3. Target Materials and Their Roles
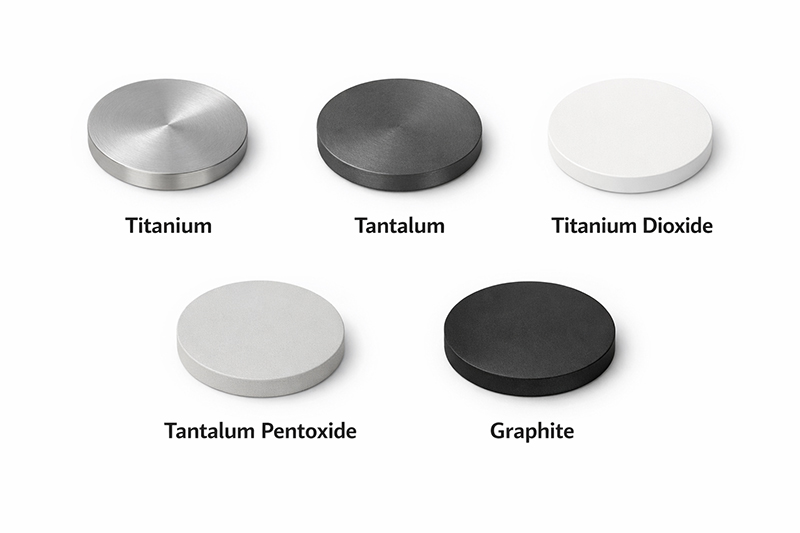
Pure titanium is the established material for osseointegration. It spontaneously forms a titanium dioxide surface layer in vivo, and osteoblasts adhere readily to this oxide. Dental implants and cementless joint components rely on titanium coatings to achieve stable bone fixation. The material must be high purity — 99.9 percent minimum — with controlled oxygen content and defect density.
Pure tantalum takes bone ingrowth a step further. Fibroblasts and osteoblasts attach even more readily to tantalum than to titanium, and the spontaneously formed tantalum pentoxide layer is exceptionally stable. Trabecular metal coatings, used extensively in revision arthroplasty, exploit tantalum’s affinity for bone. The coating can be dense for barrier applications or porous for structural ingrowth.
Titanium dioxide serves multiple functions depending on its crystal phase. Anatase, rutile, and mixed-phase coatings each exhibit different bioactivity and photocatalytic behavior. For corrosion protection on blood-contacting surfaces, dense stoichiometric TiO₂ is the goal. Phase control requires careful management of deposition temperature and oxygen partial pressure.
Tantalum pentoxide is valued for its chemical inertness and dielectric properties. It remains stable in physiological environments indefinitely, making it suitable for sensor coatings and capacitor layers in active implants. Stoichiometry control is critical — off-ratio films degrade rapidly.
Diamond-like carbon occupies a class of its own. With hardness approaching 40 gigapascals and friction coefficients below 0.2 against ultra-high molecular weight polyethylene, DLC is the material of choice for bearing surfaces and cutting tools. But DLC does not adhere well to most medical substrates directly. Chromium or silicon interlayers are typically required, and the sp³-to-sp² ratio must be controlled to balance hardness against toughness.
| Target Material | Primary Function | Typical Purity | Key Applications |
|---|---|---|---|
| Titanium (Ti) | Osseointegration | 99.9–99.99% | Dental implants, cementless joints |
| Tantalum (Ta) | Bone ingrowth | 99.95% | Trabecular metal, revision implants |
| Titanium dioxide (TiO₂) | Corrosion barrier | 99.9% | Blood-contacting surfaces, sensors |
| Tantalum pentoxide (Ta₂O₅) | Dielectric/barrier | 99.9% | Active implants, capacitor layers |
| Graphite (for DLC) | Wear protection | 99.99% | Bearing surfaces, cutting tools |
4. Process Engineering: The Difference Between Lab and Clinic
Medical coating is not simply about what you deposit. It is about how you deposit it, on what substrate, under what conditions.
Low-temperature deposition is often mandatory. Many medical substrates — polymers, some age-hardened alloys, Nitinol devices with trained shape memory — cannot tolerate elevated temperatures. Maximum processing temperature may be limited to 150 degrees Celsius or lower. This forces the use of sputtering configurations with active substrate cooling and plasma parameters optimized for minimal thermal load.
High-cleanliness processing separates medical coating from industrial coating. Particles are defects, and defects are failure initiation sites. Class 1000 cleanroom conditions are the minimum; class 100 is preferred for critical implants. ISO 14644-1 certification, particle counting during runs, and rigorous cleanroom protocols are not optional.
Surface morphology control determines clinical performance. Rough surfaces promote bone ingrowth; smooth surfaces resist thrombus formation. The same coating material can produce either outcome depending on bias voltage, working pressure, and deposition time. Achieving repeatability run to run requires closed-loop process control and thorough characterization.
Adhesion layer engineering solves the interface problem. DLC on cobalt-chrome needs chromium or silicon.
Oxides on polymers need gradient layers or plasma activation. The rule is simple: never assume direct adhesion. Verify with cross-sectional scanning electron microscopy and scratch testing, and document everything.
5. The Standards That Define Medical-Grade
Medical devices are not coated like consumer goods. They are coated like implantables — because they are.
ASTM F86 defines surface preparation and marking for metallic surgical implants. It mandates documentation of surface condition before coating and specifies acceptable cleaning and passivation methods.
ASTM F138 sets the requirements for the stainless steel most commonly used in implants. Any coating process applied to F138 substrates must not degrade the base material’s properties.
ISO 10993 governs biological evaluation. Coatings must be tested separately from substrates, and the testing must reflect the actual deposition process, the actual substrate, and the actual finished device.
ASTM F2082 applies to Nitinol devices. For coated stents and guidewires, the coating process must not alter the transformation temperature that governs device behavior.
A coating that performs perfectly in the laboratory but lacks documented evidence of compliance with these standards is not medical-grade. It is a research project. Regulatory bodies require documented evidence that the coating — as deposited, on the actual substrate, using the actual process — meets all applicable requirements.
6. Selection Summary
For load-bearing joint surfaces, DLC or titanium nitride with robust adhesion layers provides the wear resistance required for twenty-year survival. For bone interfaces, titanium or tantalum coatings with controlled roughness enable stable osseointegration. For cardiovascular devices, dense stoichiometric oxides ensure hemocompatibility and corrosion resistance. For surgical instruments, DLC preserves cutting edges and releases tissue cleanly through hundreds of sterilization cycles.
The right coating depends on the application, the substrate, and the regulatory pathway. But the principles are universal: biocompatibility first, wear and corrosion resistance second, adhesion always, and documentation throughout.
About Stanford Advanced Materials (SAM)
Stanford Advanced Materials (SAM) supplies high-purity sputtering targets for medical device coating applications. For more than thirty years, we have provided the materials that enable medical coatings — from pure titanium and tantalum to their oxides, from DLC precursors to custom alloys.
Our medical coating target materials include:
- Pure titanium, tantalum, niobium, and zirconium — 99.9% to 99.99%
- Titanium dioxide, tantalum pentoxide, niobium pentoxide, and zirconium dioxide
- Graphite targets for DLC deposition
- Custom compositions for proprietary processes
Certification of analysis, full traceability back to source, and packaging suitable for cleanroom use are available upon request.
Need assistance selecting the right target for your medical application?
Contact our medical coating specialists.




